Arterial cannulation is performed in various surgeries for continuous monitoring of blood pressure, to measure the dynamic indices of fl uid responsiveness (pulse pressure variation, systolic pressure variation, or pulse contour analysis—stroke volume variation), and for blood sampling.1 The radial artery is commonly used for arterial cannulation, followed by femoral artery. Easy accessibility and protective collateral supply of the hand are stated as reason to prefer radial artery. There are many complications associated with arterial cannulation like bleeding, ischemia, and infection. 2 Various techniques are described for arterial cannulation like ultrasound-guided, catheter-over-needle technique, and catheter-over-guidewire technique.3
The course of arterial cannulation is diffi cult in pediatric patients and thin-built patients. Inability to thread the catheter and chance of transection of the artery are unavoidable complications in this patient population. Main parameters to be analyzed while placing an arterial cannula is the depth of the radial artery, the angle at which the cannula strikes the artery, length of the path travelled by the arterial cannula before striking the radial artery. The depth of the radial artery varies with age and degree of extension of the wrist. In adults, the depth of radial artery varies from 4 to 5 mm with no extension and becomes shallower on the extension of the wrist.4 In pediatric population, the depth varies from 1 to 3 mm.5
The problem arises when the radial artery is at depth < 2 mm. In such situation, arterial cannulation becomes easy and successful by increasing the depth of radial artery by injecting saline in the subcutaneous plane or we can use the catheter-over-guidewire technique.5 Catheter-over-guidewire technique takes time and leads to soiling of surroundings with blood. Alternately we can increase the length of the path travelled by arterial cannula before striking the artery. This can be done by increasing the distance between the point of entry at the skin and the point at which cannula strikes the artery.
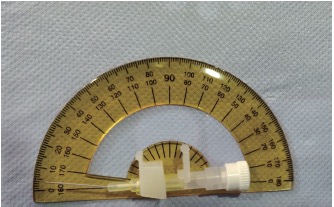
We describe a novel technique for cannulating the superfi cially located radial arteries by angulating the arterial cannula by 5–10°. This is an alternate way to decrease the angle at which cannula strikes the radial artery. Even the length of the path travelled by cannula is also indirectly increased. This is a very useful technique, in case of diffi culty to thread the artery despite hitting it and making the angle parallel to the skin to a maximum extent. This is a very common problem noticed in pediatric (neonates) and thin-built population. The angulation should be made without compromising on the sterility of the cannula (Figs. 1–2).
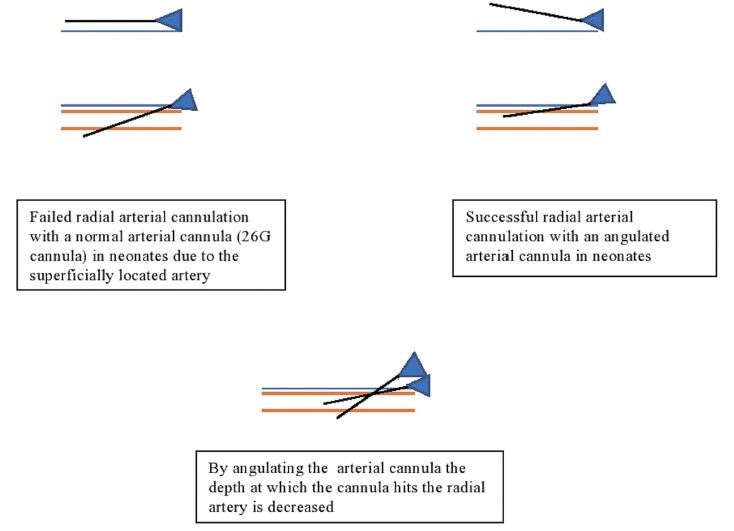
Download full-size image
Download full-size image
Angulation of arterial cannula may kink the cannula and needle. We encountered diffi culty while withdrawing the needle from the catheter. Caution needs to be executed while removing the needle and threading the cannula into the artery as the cannula might be pierced by the needle. But, good practice and slight manipulation can solve this problem. Over-angulation (> 15°) needs to be taken care of as this may break the cannula. Sterility while reshaping the catheter is another issue. We tried this technique in the pediatric population (neonates also) and the success rate of arterial cannulation improved. We used this technique in adult population where we encountered difficulty to thread the catheter despite hitting it. Further studies, may be done on this technique and arterial cannula may also be modified this way.
References
| 1 |
Marik PE, Cavallazzi R, Vasu T, Hirani A.
Dynamic changes in arterial waveform derived variables and fluid responsiveness in mechanically ventilated patients: a systematic review of the literature.
Crit Care Med 2009;37:2642–2647.
|
| 2 |
Franklin C.
The technique of radial artery cannulation. Tips for maximizing results while minimizing the risk of complications.
J Crit Illn 1995;10:424–432.
|
| 3 |
Garg R, Pandey R, Darlong V, Punj J.
Radial artery cannulation—prevention of pain and techniques of cannulation: review of literature.
Internet J Anesthesiol 2008;19.
|
| 4 |
Kang IG, Jeong WJ, Moon KM.
The relationship between radial artery depth and wrist extension angle measured by ultrasonography.
J Korean Soc Emerg Med 2013;24:279–283.
|
| 5 |
Nakayama Y, Nakajima Y, Sessler DI, et al.
A novel method for ultrasound-guided radial arterial catheterization in pediatric patients.
Anesth Analg 2014;118:1019–1026.
|