Abstract
Objective
Cardiac function analysis for Ailuropoda melanoleuca, also called giant panda, with transthoracic echocardiography has several limitations, such as limited probe position area and poor echo window. We want to determine the feasibility of transesophageal echocardiography (TEE) for cardiac examination in Ailuropoda melanoleuca.
Methods
Eight-year-old male Ailuropoda melanoleuca was anesthetized by intramuscular ketamine and followed by inhalation isofl urane with spontaneous respiration. TEE probe was inserted through mouth. Comprehensive examinations were done by two-dimensional (2D), Doppler method, 3D zoom, and 3D full volume mode for their cardiac evaluation.
Results
The structure of heart was similar to human. We found mild mitral regurgitation. Right ventricle and pulmonary artery were free of any organic lesions. We did comprehensive multiplane examination by American Society of Echocardiography/Society of Cardiovascular Anesthesia guideline, but transgastric (TG) and deep TG view were not approachable. 3D reconstruction offered high quality image and quantitative calculations. Complete examinations took less than 30 min. There was no significant hemodynamic change during probe insertion, and no oropharyngeal trauma certifi ed by dentist.
Conclusion
TEE is a reasonable semi-invasive tool for cardiac function evaluation. Though some anatomical limitations prohibited comprehensive 2D views, improvements such as 3D images help to give detailed cardiac examination.
Keywords
echocardiography, cardiovascular function, panda
Introduction
Ailuropoda melanoleuca, also known as giant panda, is a bear native to central-western and south-western China. It is a conservation reliant and endangered species recognized by International Union for Conservation of Nature. Taipei Zoo received a pair of giant pandas in 2008. They routinely had detailed annual health examination under general anesthesia.
Though we had limited experience with giant panda, we expected that with aging, they would have cardiovascular problems such as heart failure, atherosclerosis, or cardiomyopathy as other animals. In addition to that, parasite infection could also lead to cardiac dysfunction. Dirofi lariasis is a parasite infection commonly encountered in wild animals. Infectious microfi laria could be carried by mosquitos and entered host through blood and subcutaneous lymph. They usually occupied right ventricle and pulmonary artery. Symptoms ranged from none, cough, tachy-pnea, to respiratory distress. Their detection relied on direct visualization of microfilaria in the blood or positive antigen immunoassay. Ailuropoda melanoleuca is a possible host for dirofilariasis, and direct visualization of cardiac lesions could be helpful for early diagnosis and treatment.1
Transthoracic echocardiography (TTE) has been widely used for cardiac examination. There were recommended probe positions and standard views of two-dimensional (2D) TTE for dog and cat.2 Its non-invasiveness offers a convenient tool for cardiac evaluation and frequent follow-up in many different animals.3,4 It has also been used in cardiac evaluation for hibernating grizzly bears.5 To perform TTE in panda, shaving was needed to offer appropriate skin contact for echo probe, thus limited the operation field. Also, the resolution was not satisfied due to its abundant subcutaneous fat tissue. Compared to TTE, transesophageal echocardiography (TEE) often offers better image quality.3 Detailed functional analysis such as ventricular mass calculation, Doppler flow measurement, speckle tracking, or 3D image acquisition needs superb image resolution for further calculation. Therefore, TEE should be better than TTE in elaborated cardiac examination.
TEE is semi-invasive, which requires sedation or general anesthesia for probe insertion. We evaluated the feasibility of TEE under general anesthesia, the first time ever in giant panda.
Methods
Male giant panda, weight 125 kg, aged 8 years old, was sedated by intramuscular ketamine 1 g. Intubation was done by direct laryngoscope No. 5 with 8 mm I.D. and 9 mm I.D. endotracheal tube connected together. Endotracheal tube was fixed at a depth of 60 cm from inscisor. End-tidal CO2 was used to monitor accurate endotracheal tube position. Its value was also an indicator for adequate ventilation. Saturation was monitored by pulse oximeter on their tongue. Blood pressure was measured by blood pressure cuff on their forelimbs. Intravenous catheter was inserted on his neck. An infusion pump was used to keep adequate intravenous volume supplement. General anesthesia with spontaneous respiration was maintained by isoflurane. TEE probe (iE33 xMATRIX with X7-2t transducer; PHILIPS, Amsterdam, Netherlands) was inserted through mouth for examination. We did comprehensive multiplane TEE examination recommended by the American Society of Echocardiography (ASE) and the Society of Cardiovascular Anesthesia (SCA) guideline.6,7 3D Full-volume and 3D zoom were used to obtain image, and quantitative calculation was done by analyzed using Q lab software (Philips Medical Systems, Andover, Massachusetts). Dentists did oral examination and cleaning after TEE examination.
Results
The probe was inserted without difficulty. Baseline heart rate and blood pressure were 75/min and 132/83 mmHg. There was no significant increase (less than 10%) in heart rate and blood pressure after TEE probe insertion. The depth to acquire four-chamber view was about 50-55 cm. The structure of heart was similar to human.
We subsequently obtained mid-esophageal (ME) 5-chamber view, ME 4-chamber view, ME mitral commissure view, ME 2-chamber view, ME long-axis view, ME aortic valve long axis view, ME ascending aorta long axis view, ME ascending aorta short axis view, ME right pulmonary vein view, ME aortic valve short axis view, ME right ventricular inflow-outflow view, ME modified bicaval tricuspid view, ME bicaval view, ME atrial appendage view, upper esophageal (UE) right and left pulmonary vein view, UE aortic arch long axis view, UE aortic arch short axis view, descending aorta short axis view, and descending aorta long axis view. After several attempts, we failed to acquire transgastric (TG) images and deep TG (DTG) images.
There was no regional wall motion abnormality from either ME 4-chamber or ME 2-chamber view. We did Simpson Bi-plane method, and the left ventricular ejection fraction (LVEF) was 48%. Mild mitral regurgitation with central jet was noted, and there was no evidence of diastolic dysfunction. Right ventricle and pulmonary artery were free of any parasite or organic lesions. No atherosclerosis of aorta was noted. Quantitative measurements taken by 2D and Doppler method were shown in Table 1.
Download full-size image
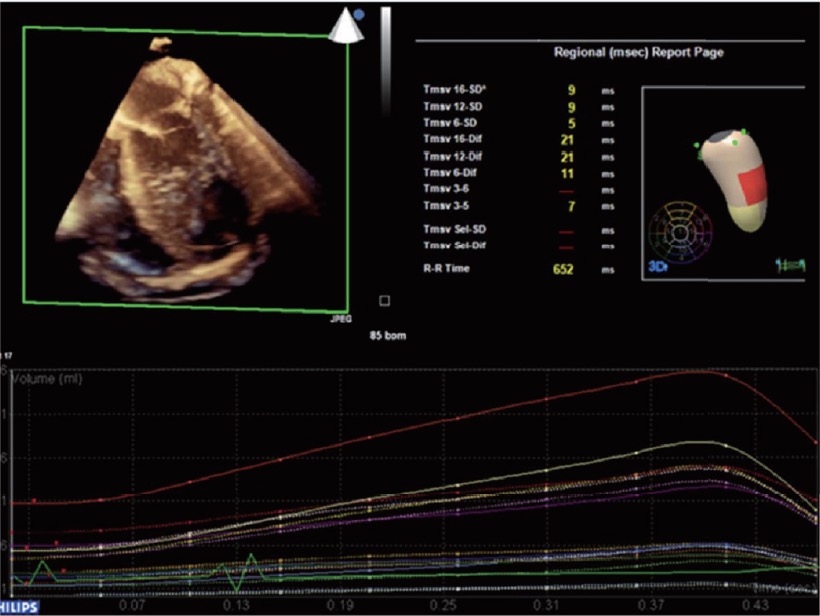
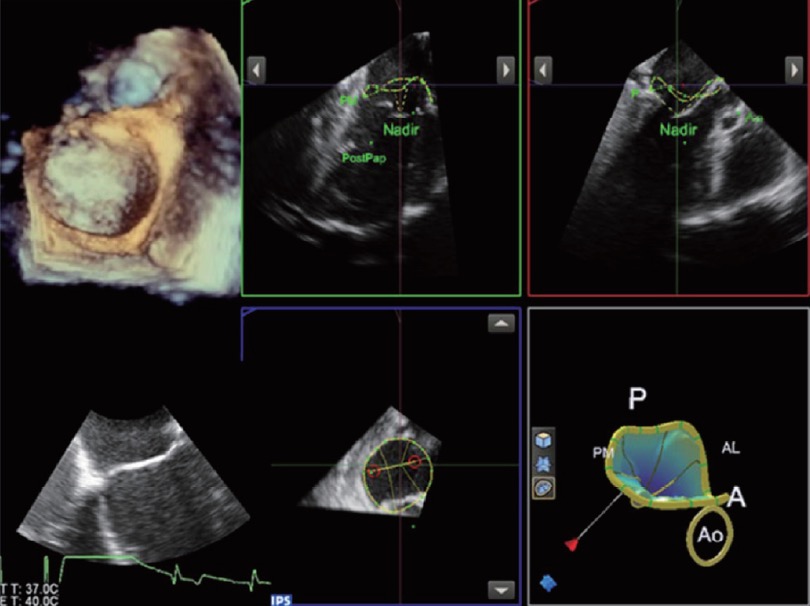
3D full volume reconstruction for left ventricle showed synchronized contraction and good contractility (Fig. 1). LVEF from 3D calculation was 52%. The red territory at lateral wall was due to insufficient image data. Aortic valve and mitral valve enface view was shown in Fig. 2. The relationship of aorto-mitral angle, papillary muscle, and chordae chordae tendinae was displayed in the simplified model.
Download full-size image
Download full-size image
The duration of examination was about 20 min. No oropharyngeal trauma was noted after the procedure.
Discussion
Complete TEE examinations were performed smoothly for giant panda first time ever in less than 25 min. This giant panda have fair ventricular contractility, mild central mitral regurgitation, no evidence of diastolic dysfunction. Major blood vessels looked normal. The resolution for the image was acceptable, and no adverse event was noted during the examination.
Cardiac echocardiography grounded on the basis of anatomy. Previous reports from autopsy showed that Ailuropoda melanoleuca had a vertical heart in the mediastinum of their thorax. Its axis strode from right anterior to left posterior. The heart apex was posteriorly deviated. Its morphology was oval-shaped, similar to canine. There were four chambers in the heart. Right atrium was larger than left atrium, and left ventricle was more muscular than right ventricle. Right side atrioventricular valves had three leaflets, and left side atrioventricular valves had two leafl ets, which connected to chordae and papillary muscles. All the major vessels in the heart base were covered in the pericardium. Right pulmonary artery was around 4.0 cm inside its pericardium, whereas aorta was 3.3 cm and pulmonary vein was 1.2 cm. The length of these vessels could vary signifi cantly from individual to individual.8
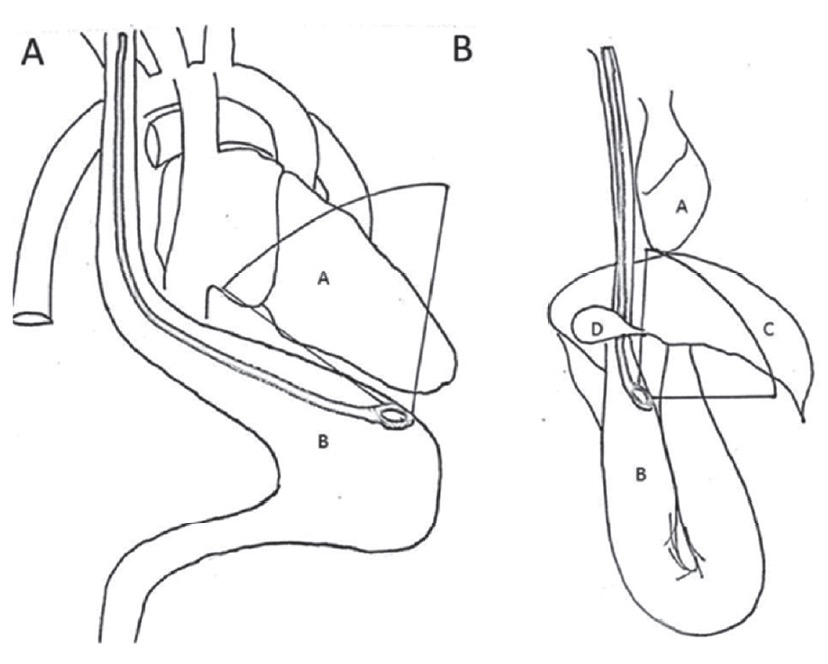
The ASE/SCA recommended 28 views for comprehensive TEE examination.6,7 All the views could be obtained with slight probe adjustment. However, DTG and TG view were not feasible in both pandas. DTG view was obtained by advancing TEE probe to the stomach and antefl exed the probe. It is primarily used for diagnosis of aortic valve and left ventricular outflow tract pathology. Due to the alignment, it is especially useful for Doppler interrogation of aortic outfl ow. The relative position of gastrointestinal tract and heart is different from human to panda (Fig. 3). In panda, their stomach is sac like with a U turn. Their liver occupies the subphrenic region, and the left lobe is larger than human, which covers the stomach. Furthermore, the heart apex in panda is posteriorly deviated. Combining all the above factors, there was no contact between stomach and heart apex, which prohibits for DTG view acquisition (Fig. 4).
Download full-size image
(A) TEE probe position for deep transgastric (DTG) view in human.
(B) In panda, stomach is covered by liver, and the shape is a U sac. TEE probe in the gastric region is far from cardiac apex, thus incapable to get a DTG view.
A: heart; B: stomach; C: liver; D: gall bladder.
Download full-size image
We used 3D TEE probe for the examination this time. Live 3D and 3D zoom mode gave us an easy and accurate way to evaluate left atrioventricular valve on the spot. It was more straight-forward than 2D images, and by rotating the plane, we could observe the valve from either enface or up-side down. For full volume images, the probe scanned through larger angles, and acquired more extensive information. The images would be assembled by the computer. Because the panda had spontaneous respiration, it was hard to hold their breath and got a fl awless full volume image. Full volume image of the heart offers better estimation of ventricular function and valve calculation.9 With the improvement of echocardiography, we hope image acquisition will be easier and faster for on spot evaluation.
In conclusion, TEE is a reasonable choice for cardiac examination in giant panda. It is semi-invasive, offers better resolution than TTE, and saves the needs for shaving. Our examination for two giant panda showed excellent image acquisition without any complications. Due to the remote distance from stomach and cardiac apex, DTG view is not available. Other comprehensive 2D views and 3D TEE images are comparable to human beings with slight difference.
Acknowledgments
The authors acknowledge Taipei Zoo for collaboration of this examination.
Author Contribution
Category 1
(1) Conception and design: Yi-Chia Wang; Wei- Zen Sun.
(2) Acquisition of data: Chi-Hsiang Huang; Man-Ling Wang.
(3) Analysis and interpretation of data: Yen-Hsu Lai.
Category 2
(1) Drafting the article: Yi-Chia Wang.
(2) Revising article for intellectual content: Jun-Cheng Guo; Pao-Jung Wang.
Category 3
Final approval of the completed article: Chi- Hsiang Huang.
Conflicts of Interest
None.
References
| 1 |
Lan J, Fu Y, Yang Z, et al.
Treatment and prevention of natural heartworm (Dirofilaria immitis) infections in red pandas (Ailurus fulgens) with selamectin and ivermectin.
Parasitol Int 2012;61:372-374.
|
| 2 |
Thomas WP, Gaber CE, Jacobs GJ, et al; Echocardiography Committee of the Specialty of Cardiology, American College of Veterinary Internal Medicine.
Recommendations for standards in transthoracic two-dimensional echocardiography in the dog and cat.
J Vet Intern Med 1993;7:247-252.
|
| 3 |
Schwarz ER, Pollick C, Meehan WP, Kloner RA.
Evaluation of cardiac structures and function in small experimental animals: transthoracic, transesophageal, and intraventricular echocardiography to assess contractile function in rat heart.
Basic Res Cardiol 1998;93:477-486.
|
| 4 |
Leroux AA, Farnir F, Moonen ML, Sandersen CF, Deleuze S, Amory H.
Repeatability, variability and reference values of pulsed wave Doppler echocardiographic measurements in healthy Saanen goats.
BMC Vet Res 2012;8:190.
|
| 5 |
Nelson OL, McEwen MM, Robbins CT, Felicetti L, Christensen WF.
Evaluation of cardiac function in active and hibernating grizzly bears.
J Am Vet Med Assoc 2003;223:1170-1175.
|
| 6 |
Hahn RT, Abraham T, Adams MS, et al.
Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists.
J Am Soc Echocardiogr 2013;26:921-964.
|
| 7 |
Hahn RT, Abraham T, Adams MS, et al; American Society of Echocardiography; Society of Cardiovascular Anesthesiologists.
Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists.
Anesth Analg 2014;118:21-68.
|
| 8 |
Yong-Chen Wang [wáng yǎng zhèng].
Anatomy and Dissection of Giant Panda [dà xióng māo jiě pǒu].
China: Science Publication; 1986:291-298.
|
| 9 |
Nessly ML, Bashein G, Detmer PR, Graham MM, Kao R, Martin RW.
Left ventricular ejection fraction: single-plane and multiplanar transesophageal echocardiography versus equilibrium gated-pool scintigraphy.
J Cardiothorac Vasc Anesth 1991;5:40-45.
|