Abstract
Background: A self-infl ating bag (SIB) is an essential device for pulmonary resuscitation in emergencies. However, it is difficult for a rescuer to accurately predict a tidal volume (TV) delivered by a SIB to patient.
Objective: The objective of this study was to evaluate TV values delivered by a SIB with various compression methods.
Methods: A total of 33 participants were enrolled in this study. Anterior, middle, and posterior points were marked on the surface of the SIB to guide participants to place their fingers. This was connected to a gas-flow analyzer and a test lung to measure the TV. Participants were asked to squeeze the SIB with onehanded and two-handed compression at anterior, middle, and posterior points.
Results: The TV was the largest when the bag was squeezed with two-handed compression at the middle points (578 ± 21 mL). It was the smallest when the bag was squeezed with one-handed compression at the anterior point (311 ± 15 mL). Except that the TV with one-handed compression at the middle point and the TV with two-handed compression at the posterior points were similar, all other TV values were signifi cantly different from each other (all P < 0.001).
Conclusion: The TV delivered by a SIB could differ greatly depending on the compression points and whether one or two hands are used. Therefore, a rescuer should choose an appropriate compression method considering patient’s physical characteristics and medical conditions.
Keywords
equipment design, resuscitation, tidal volume
Introduction
A self-infl ating bag (SIB) is an essential device in emergencies that provides basic life support. The America Heart Association guidelines for cardiopulmonary resuscitation (CPR) recommends that a tidal volume (TV) of approximately 500–600 mL should suffice and that rescuers should avoid excessive ventilation during adult CPR.1 The optimal TV for pediatric CPR is currently unknown. However, rescuers should also avoid excessive ventilation and give just enough TV to make the chest rise.2
Because both insufficient and excessive ventilation during CPR are harmful, it is important to deliver an adequate TV. However, the TV delivered by a SIB can differ widely depending on a rescuer’s personal training experience and compression method.3-7 Therefore, it is diffi cult to predict the TV delivered by a SIB to a patient in emergencies.
We hypothesize that the TV delivered by a SIB could differ depending on the compression points and whether one or two hands are used. Thus, we marked several compression points on a SIB to guide participants to place their fingers and then evaluated TV values delivered by the SIB with either one-handed or two-handed compression.
Methods
This study was approved by the Institutional Review Board (No. 2017-04-007) and registered to the Korea Clinical Research Information Service (No. KCT0004091). Written informed consent was obtained from each participant.
A SIB (Rescu-7 adult manual resuscitator 1,500 mL, Galemed Corporation, Taiwan) was designed with anterior, middle, and posterior compression points (A, A’, B, B’, C, and C’). These points were marked at a distance of 2.5 cm up and down from the midline of the bag (Figure 1). The SIB was connected to a gas-flow analyzer (VT mobile, Fluke Biomedical, Cleveland, OH, USA) for measuring the TV. It was then connected to an adult test lung (Maquet adult test lung 1 L, MAQUET Medical Systems, Wayne, NJ, USA) for physiological simulation (Figure 2).
Download full-size image
Download full-size image
Participants enrolled in this study were doctors, senior medical students, and nurses. The size of a dominant hand was measured from the middle fingertip to the distal skin crease at the wrist. To deliver ventilations, participants were guided to put the first finger at the marked point and the third finger on the opposite side by placing the rest of the fingers naturally on the surface of the bag. Next, they were instructed to squeeze the bag using all fingers until the first finger contacted the middle finger. Each ventilation was carried out for one second with the rate at ten per minute.
Participants first squeezed the bag with onehanded compression at A, B, and C points (Figure 3A) and then squeezed the bag with two-handed compression at AA’, BB’, and CC’ points simultaneously (Figure 3B). Each of them squeezed the bag ten times for each of six kinds of compression methods (A, B, C, AA’, BB’, and CC’), giving a total of 60 ventilations. If needed, sufficient rest was allowed.
Download full-size image
Data were analyzed using SPSS (IBM SPSS statistics 2.0 for Windows; IBM Corp., Armonk, NY, USA). One-way analysis of variance (ANOVA) was performed for TV values obtained with one-handed or two-handed compression. The TV values delivered by six kinds of compression methods (A, B, C, AA’, BB’, and CC’) were compared with each other on a one-to-one basis using Student’s t-test. Spearman’s correlation analysis was performed to find correlations between the participants’ characteristics and TV values. Statistical signifi cance was set at P < 0.05.
Results
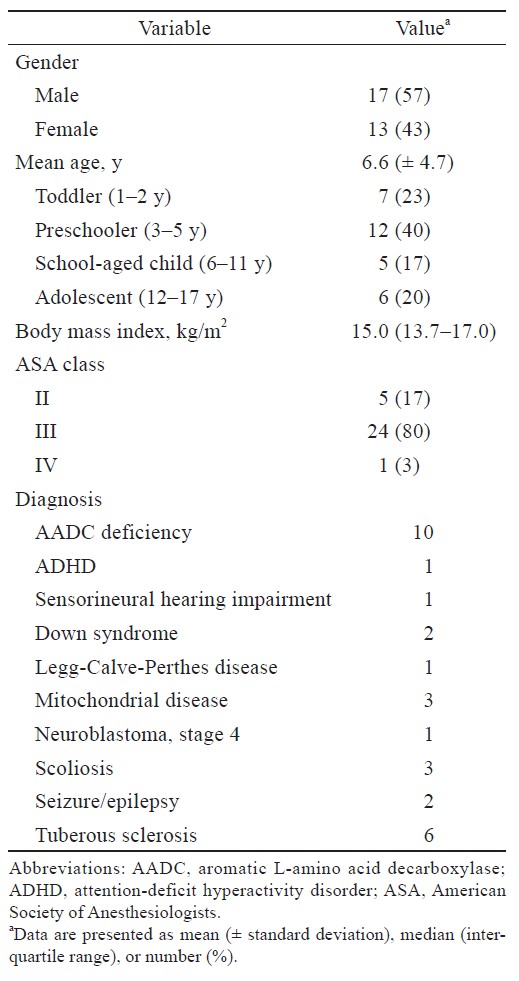
A total of 33 participants were enrolled in this study (Table 1). A total of 330 TV values (33 participants × ten ventilations) were collected for each compression method.
Download full-size image
For either one-handed or two-handed compression, the TV was the largest when the bag was compressed at the middle points. The next largest TV was obtained when the bag was compressed at the posterior points. The TV was the smallest when the bag was compressed at anterior points (i.e., B > C > A and BB’ > CC’ > AA’, all P < 0.001). The TV values obtained with two-handed compression were significantly greater than those with one-handed compression when the bag was squeezed at the same midline location (i.e., AA’ > A, BB’ > B, CC’ > C, all P < 0.001) (Table 2).

Download full-size image
All TV values were significantly different from each other (all P < 0.001), except for the TV with one-handed compression at point B and the TV with two-handed compression at point CC’. The TV was the largest when the bag was squeezed with two-handed compression at point BB’ (578 ± 21 mL). It was the smallest when the bag was squeezed with one-handed compression at point A (311 ± 15 mL). The overall result for TV values was BB’ > B = CC’ > AA’ > C >A.
Among 330 TV values obtained with two-handed compression at point BB’, the largest value was 619 mL while the smallest value was 534 mL. Of them, 271 (82.1%) TV values were within 500–600 mL.
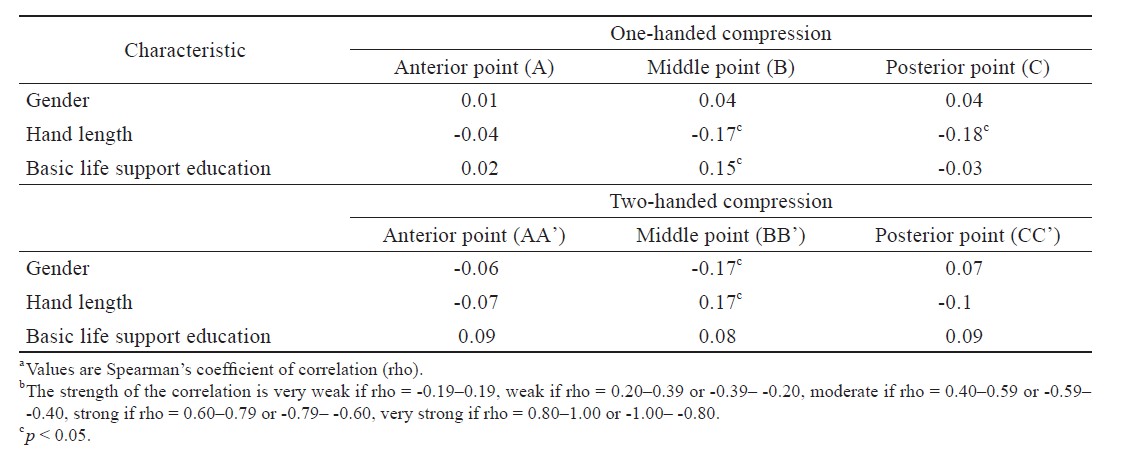
The analysis of correlations between the participants’ characteristics (gender, hand length, basic life support education) and TV values showed very weak Spearman’s coefficient of correlation (rho) between -0.19 and 0.19 (Table 3).
Download full-size image
Discussion
Although several studies have reported that it isimpossible to deliver the accurate TV using a conventional SIB,3,5 a SIB is still the most commonly usedfirst-line respiratory assist device during emergency resuscitation or intensive-care management. We hypothesize that the TV delivered by a SIB dependson which point is compressed and whether one ortwo hands are used. We marked several compression points on a SIB to guide participants about where toplace their fingers and obtained TV values using various compression methods. This study showed that the TV delivered by a SIB could have large differences depending on the compression method used.
The purpose of assisted ventilation during CPR is to maintain adequate oxygenation and eliminate CO2. The America Heart Association guidelines for CPR suggest that a TV and respiratory rate lower than normal are needed during CPR. Excessive ventilation can be harmful because it causes gastric inflation, increases intrathoracic pressure, decreases venous return, and diminishes cardiac output and survival. A TV of approximately 500–600 mL has been recommended to produce a visible chest rise in adults.1
In children, an appropriate TV for CPR has not been established yet. As with adult CPR, excessive ventilation for children can also be harmful. Thus, a TV that produces a visible chest rise may suffice. Using an adult SIB is recommended for older children and adolescents because smaller bags may not deliver an effective TV or may require longer inspiratory time.2
Theoretically, the TV of 500–600 mL for adult CPR can be delivered by squeezing a one-liter SIB to about one-half to two-thirds of its volume or a two liter SIB to about one-third of its volume. However, the TV delivered by a SIB can differ greatly depending on a rescuer’s personal training experience, compression technique, and a SIB manufacturer. Lee et al.3 have analyzed a TV delivered by a conventional compression method using a 1.6 L SIB. They found that a TV delivered by two-handed compression was significantly greater than that delivered by one-handed compression. Two-handed half compression gave the smallest TV out of all methods. They concluded that the TV delivered by a SIB showed large differences and that a SIB was not a suitable device for accurate ventilation. McCabe and Smeltzer6 have also reported that a TV delivered by two-handed compression is significantly greater than that delivered by one-handed compression.
To reduce such differences, Cho et al.8 have suggested markers when using a SIB to guide placement of fingers on the bag surface. Participants were instructed to place their five fingers of one hand on these markers followed by squeezing the bag until the thumb and the third finger made contact. This method delivered more sustained TV than a conventional compression method. Park et al.9,10 have also suggested the use of compression markers on a SIB to deliver a desired TV.
Since the conventional compression method has shown large differences in TV values, we modified and used the compression method proposed by Cho et al.8 to deliver a regular and sustained TV. We marked several compression points on a SIB and measured TV values delivered by one-handed and two-handed compression. For each compression point, TV values were relatively constant with a low standard deviation. However, they showed large differences compared to those obtained with other compression points.
For either one-handed or two-handed compression, the TV was the largest when the bag was compressed at the middle points. The next largest TV was obtained when the bag was compressed at the posterior points. The TV was the smallest when the bag was compressed at the anterior points. We also showed that two-handed compression delivered more TV than one-handed compression when the bag was squeezed at the same midline location.
Therefore, rescuers should know the amount of TV according to each compression point with one-handed or two-handed compression. They should be able to choose the best method depending on the individual patient. For example, in our study, two-handed compression at the middle points (BB’) delivered the largest TV and seemed to be the most suitable way to deliver a TV of 500–600 mL as recommended by adult CPR guidelines with 82.1% accuracy. If a rescuer uses other compression methods, sufficient TV may not be provided in a large adult. Especially, one-handed compression at the anterior point (A) delivered a TV of 312 ± 15 mL, which was only 54% of a TV by two-handed compression at the middle points (BB’). So if a rescuer has no choice but to use one hand, he or she should compress the middle point of the bag to deliver the most suitable TV in a large adult.
One the other hand, when performing CPR for an older child, other compression methods should be considered to deliver the proper TV. There is no guideline describing the appropriate TV capacity in terms of the size or weight of a child. In general, 6–7 mL/kg of a TV produces a visible chest rise.1 According to this, if the expected weight of an older child is 50 kg, the recommended TV is 300–350 mL. Therefore, one-handed compression at the anterior point (A) could be the most suitable one for delivering this amount of TV. If a slightly more amount of TV is required, one-handed compression at the posterior point (C) could be used next.
This study has several limitations. First, in the simulation experiment, the SIB was directly connected to a gas-flow analyzer and a test lung. Such a setting might be different from the actual emergency medical situation. Second, in our study, the TV obtained with one-handed compression was too small for adult CPR. This result is different from previous studies showing that one-handed compression could deliver a TV of 500–600 mL.3,8 Such difference might be due to different sizes and materials of the SIB from different manufacturers. It might also be due to an error between gas-flow analyzers or participants’ physical characteristics. Further studies are needed to clarify this issue.
In conclusion, the TV delivered by a SIB could differ greatly depending on the compression points and whether one or two hands are used. Therefore, a rescuer should choose an appropriate compression method considering the patient’s physical characteristics and medical conditions.
Acknowledgments
This work was supported by a research grant from Jeju National University Hospital in 2017.
References
| 1 |
Berg RA, Hemphill R, Abella BS, et al.
Part 5: adult basic life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular
Circulation. 2010;122(18 suppl 3):S685-S705.
|
| 2 |
Berg MD, Schexnayder SM, Chameides L, et al.
Part 13: pediatric basic life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.
Circulation. 2010;122(18 suppl3):S862-S875.
|
| 3 |
Lee HM, Cho KH, Choi YH, Yoon SY, Choi YH.
Can you deliver accurate tidal volume by manual resuscitator?
Emerg Med J. 2008;25(10):632-634.
|
| 4 |
Elling R, Politis J.
An evaluation of emergency medical technicians’ ability to use manual ventilation devices.
Ann Emerg Med. 1983;12(12):765-768.
|
| 5 |
Augustine JA, Seidel DR, McCabe JB.
Ventilation performance using a self-inflating anesthesia bag: effect of operator characteristics.
Am J Emerg Med. 1987;5(4):267-270.
|
| 6 |
McCabe SM, Smeltzer SC.
Comparison of tidal volumes obtained by one-handed and two-handed ventilation techniques.
Am J Crit Care. 1993;2(6):467-473.
|
| 7 |
Davidovic L, LaCovey D, Pitetti RD.
Comparison of 1- versus 2-person bag-valve-mask techniques for manikinventilation of infants and children.
Ann Emerg Med. 2005;46:37-42.
|
| 8 |
Cho YC, Cho SW, Chung SP, Yu K, Kwon OY, Kim SW.
How can a single rescuer adequately deliver tidal volume with a manual resuscitator? An improved device for delivering regular tidal volume.
Emerg Med J. 2011;28(1):40-43.
|
| 9 |
Park SO, Lee KR, Baek KJ, Hong DY, Shim HW, Shin DH.
Novel target volume marked adult bag to deliver accurate tidal volume for paediatric and adolescent resuscitation.
Resuscitation. 2011;82(6):749-754.
|
| 10 |
Park SO, Lee KR, Baek KJ, Shim HW, Hong DY.
Evaluation of a novel paediatric self-inflating bag to improve accuracy of tidal volumes delivered during simulated advanced paediatric resuscitation.
Resuscitation. 2012;83(1):101-106.
|