Abstract
Background
With the increase in the number of people exposed to anesthetic gases, there is a critical need to examine the prevalence of neurotoxic symptoms in these individuals using reliable tools. The aim of this study was to evaluate the psychometric characteristics of EUROQUEST questionnaire and to measure the rate of neurotoxic symptoms in the anesthesiology personnel.
Methods
This research was a cross-sectional study. This study was a cross-sectional one. Participants included 404 personnel of the operating room in western Iran. EUROQUEST questionnaire was translated into Persian and used to measure the rate of neurotoxic symptoms. Reliability of the questionnaire was examined by Cronbach’s alpha, while face and construct validities were evaluated using SPSS 16 (SPSS Inc., Chicago, IL, USA) and AMOS 18 (IBM, Chicago, IL, USA) software.
Results
The results indicated that EUROQUEST questionnaire had acceptable reliability and validity. The most prevalent symptoms were observed in memory and concentration, fatigue, and sleepiness. The prevalence of fatigue was higher than other dimensions, with 28% of participants in the third and fourth quartiles. Also, there was no relationship between symptoms and work experience.
Conclusions
EUROQUEST questionnaire can be applied in studies of the neurotoxic symptoms. The study of the prevalence of symptoms also indicated that most participants complained about memory and concentration, fatigue, and sleepiness, and these symptoms were observed in all individuals regardless of their work experience.
Keywords
anesthesiology, euroquest, neurotoxic, operation room, psychometric
Introduction
Healthcare is one of the fastest growing businesses. Health workers face risks such as leakage of anesthetic gases, sterilant gases, solvents, and disinfectants in addition to physical injuries including needle stick injuries, back injuries, and workplace stressors.1
Hospital personnel are exposed to anesthetic gases in various wards of health centers such as operating and recovery rooms.2 Epidemiological studies have shown that exposure to low-level anesthetic gases can have serious effects on the health of individuals.3,4 Inhalational anesthetics are evaporating and non-flammable liquids that have been used in health centers for more than a hundred years. These drugs are liquid and are administered to the patients by the evaporators in a gas form. Sevoflurane, halothane, and isoflurane are the most commonly used substances.5
The number of people exposed to anesthetic gases is increasing with the increase in the number of health care centers.6 Gas leakage from the anesthetic machine, lack of a scavenging system, anesthetic spillage, exhalation of patients, and absence of conduction of anesthetic waste gases outside the operating room are among the causes of contamination of air with anesthetic gases in the operating rooms.7
The risk of hepatitis and renal disease has also increased among staff exposed to this substance.3 Effects on the central nervous system because of chronic contact with anesthetic gases, followed by headache, fatigue, nausea and vomiting, sleepiness, dizziness, eye irritation and redness, oral and throat irritation, and respiratory tract irritation, have been observed among staff exposed to anesthetic gases.3,5,6,8
According to researchers, investigating the effects of exposure to anesthetic gases and providing appropriate methods to prevent and reduce the harmful effects of these gases are very important;5 therefore, sensitive and applicable screening tests, such as a questionnaire, are needed to detect the harmful effects at an early stage in order to prevent the development of encephalopathy.9
EUROQUEST questionnaire was designed in 1992 by a group of experts (EURONEST) (European neurotoxic solvents toxicology group) in order to perform neurotoxicity epidemiologic studies.10 High sensitivity, combining different aspects of the questionnaire, and covering all neurological symptoms are among the advantages of this questionnaire.11
Despite the difficulties in interpreting the self-report data, the questionnaire of neurological symptoms was successfully applied in epidemiologic studies.12 EUROQUEST questionnaire was provided in different languages and cultures based on the previous questionnaires, research, and expertise of the EURONEST on chronic solvent encephalopathy in order to standardize neuro-toxicological methods.9 Reliability of the French version of EUROQUEST questionnaire was evaluated by Rouch et al.10 Cronbach’s alpha coefficient of this questionnaire was more than 0.6 for all sections except for sleep disorders. Another study examined the reliability of the Spanish version of EUROQUEST questionnaire13 and indicated that Cronbach’s alpha coefficient in this questionnaire was higher than 0.7.
Knowing the importance of the issue of exposure to anesthetic gases and considering the unique features of the current questionnaire, preparing and validating the Persian version of this questionnaire can have a useful and effective role in evaluating the neurotoxic symptoms in the operating room personnel. Therefore, the aim of this study was to investigate the reliability and validity of EUROQUEST questionnaire in the anesthesiology staff.
Methods
This descriptive-analytic study was conducted to prepare the Persian version of EUROQUEST questionnaire for the anesthesiology staff and investigation incidence of neurotoxic symptoms. In this study, linguistic validation, content validity, construct validity, and Cronbach’s alpha coefficient were used to assess the validity and reliability of EUROQUEST questionnaire. The sample consisted of 404 personnel who were employed in hospitals in western Iran and selected by simple random sampling method. This study was conducted from January to May 2020 for 5 months.
Inclusion criteria were at least one year of experience in the operating room and continuous presence (without long-term leave) in the last three months at work. Exclusion criteria in this study were having a second job, having a physical or mental illness, and taking psychiatric medications at the time of the study (which participants were asked to self-report). All of them were people who only worked in the operating rooms of hospitals and did not work in other wards. All participants in this study were shift worker, and all of them answered the questionnaire in the morning shift and in the middle of working hours.
EUROQUEST Questionnaire
Chronic neurotoxic effects were evaluated using the 59-item English version of EUROQUEST questionnaire which consists of six parts: neurological (questions 1–12), psychosomatic (questions 13–26), mood (questions 27–37), memory and concentration (questions 38–47), fatigue (questions 48–54), and sleep disorders (questions 55–59). Each question contains four options of “never or rarely”, “sometimes”, “often or usually”, and “always or most often.”9,14
Determining the Members of the Panel of Experts
Panel members included 10 experts in the field of industrial and organizational psychology as well as expert staff (operating room personnel with a high work experience).
Preparing the Persian Version of EUROQUEST Questionnaire
As the first step, the original version of EUROQUEST questionnaire was translated from English to Persian using the standard version of the questionnaire, and it was then re-translated. In this method, the original version of the questionnaire was first translated from English to Persian by two English language experts independently of each other. Then the inverse translation of the questionnaire was performed by two independent translators familiar with the specialized topics. Finally, in order to ensure that both English versions are equivalent and have the same semantic load, the translated version was compared with the original one and after we selected appropriate semantic and idiomatic equivalents for the words and made changes to fit the questionnaire with the operating room occupation, the final version was prepared.
Evaluating the Questionnaire Validity
In this study, the content validity ratio (CVR) was evaluated based on the method presented by Lawshi. The questionnaire was given to a group of experts who were asked to accurately determine their opinions on each item in three scales of “necessary,” “useful, but unnecessary” and “unnecessary.” After we collected expert opinions, the CVR was calculated based on the Lawshi formula in order to quantitatively evaluate the content validity, and also to ensure that the most significant and relevant content had been selected.
In which ne indicates the number of participants who have selected the “necessary” item, and N represents the total number of expert people.
After we determined and calculated the CVR, content validity index (CVI) as well as average CVI (S-CIV/AVE) were used to ensure that the questions had been designed to measure the content in the best way. In order to examine the CVI, three criteria of simplicity, specificity (relevance), and resolution were separately examined in a four-point (Likert) scale for each item by the panel of experts. Eventually, the CVI score was calculated by division of the sum of positive scores for each item ranked 3rd and 4th (the highest score) by the number of experts.
Hyrkäs et al.15 have recommended 0.79 and higher values for accepting the items based on CVI score. If the CVI is between 0.70 and 0.79, the term needs to be modified and revised, and if the CVI score is less than 0.70, the term will be deleted. Then, based on the mean of CVI of all questions, the average CVI of the questionnaire (S-CVI/AVE) was also calculated. The results showed that all questions had acceptable CVR and CVI.
Ethical Statement
This research was approved by ethical in research committee of Hamdan University of Medical Science and registered with this code: IR.UMSHA.REC.1396.900.
Results
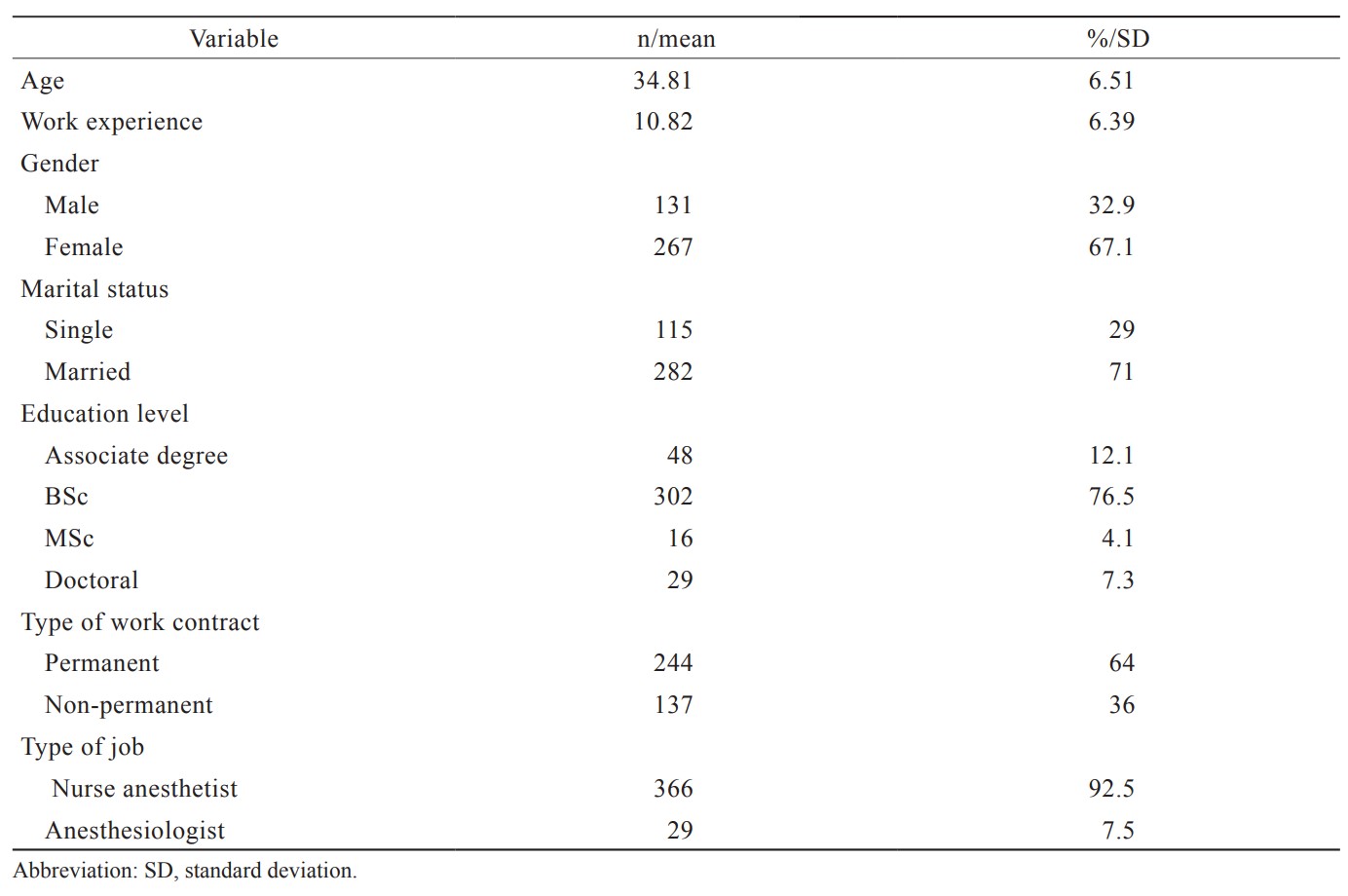
Selected demographic characteristics of the sample were summarized in Table 1.
Download full-size image
Confirmatory Factor Analysis
The 6-factor model was investigated. To test the fit between the data and the underlying theoretical construct, a confirmatory factor analysis was performed. Several fit indices were calculated, based on recommendations.16,17 These indices are displayed in Table 2. As can be seen, an overall satisfactory model fit was achieved. Factor score weight for each subscale is displayed in Table 3. Also in the last column of Table 3, the reliability of subscales with Cronbach’s alpha was estimated.

Download full-size image

Download full-size image
Download full-size image
Download full-size image
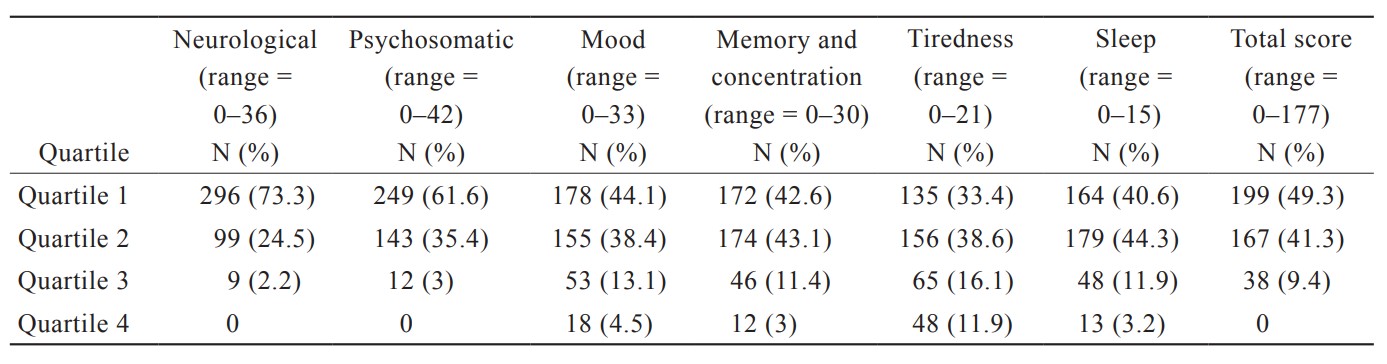
In Table 4, the scores for each domain are quartiled, and the number of people in each quartile is represented. In order to enable the ranking of individuals in each subscale and to compare the severity of symptoms in participating in the different subscales, a quadratic was used. The maximum score to be obtained in each subscale was divided into 4 equal parts, and quartile 1 refers to the first part, quartile 2 refers to the second part, quartile 3 refers to the third part, and quartile 4 refers to the fourth part. In the case of neurological subscale, 73.3% of the participants had a score of 0 to 9 (quartile 1), 24.5% of the participants had a score of 10 to 18 (quartile 2), 2.2% of the participants had a score of 19 to 27 (quartile 3), 0% of the participants had a score of 28 to 36 (quartile 4). The same goes for other subscales. According to Table 4, neurological, psychosomatic, and mood symptoms were the most prevalent in the first quartile, and the symptoms of memory and concentration, tiredness, and sleepiness were the most prevalent in the second quartile. Prevalence of tiredness was higher than other dimensions, so that 28% of participants were in the third and fourth quartiles of this dimension.
Download full-size image
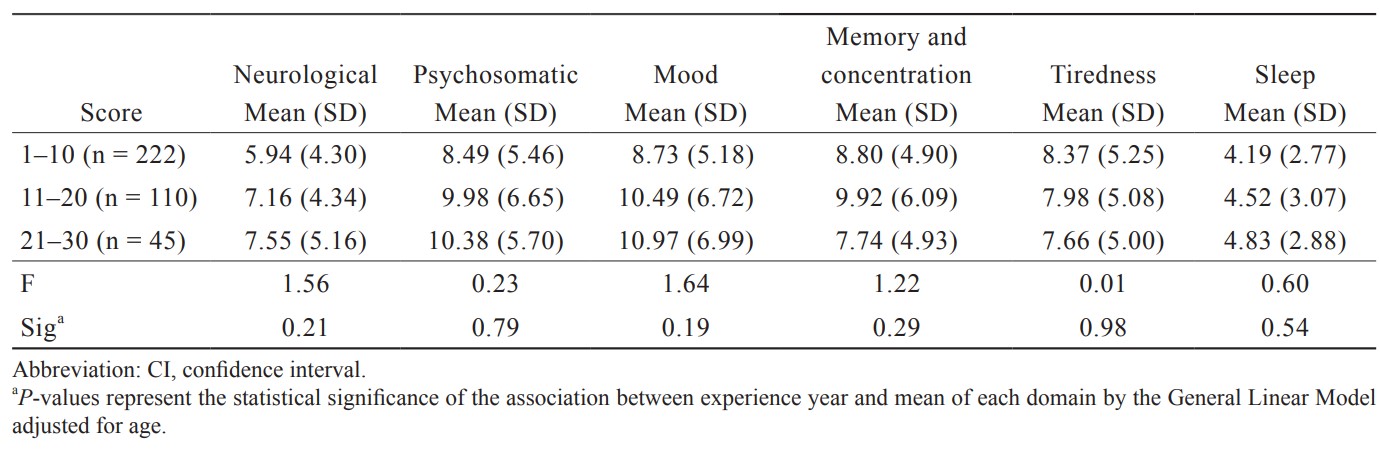
Table 5 shows the mean of each domain in terms of work experience The results indicate that there are no significant differences between the three groups of work experience in any of the domains.
Download full-size image
Discussion
The present study was conducted to develop a Persian version of the 59-item EUROQUEST questionnaire and investigate its psychometric properties along with the evaluation of the prevalence of neurotoxic symptoms in the anesthesiology staff. The findings of this study show that EUROQUEST questionnaire has an appropriate and acceptable validity index. Also, reliability of EUROQUEST questionnaire was reported 0.82, 0.83, 0.92, 0.89, 0.89, and 0.66, respectively by calculating Cronbach’s alpha for neurological, psychosomatic, mood, memory and concentration, tiredness and sleepiness dimensions. All questionnaire dimensions were higher than the standard value (0.7), except sleepiness.
Having evaluated the reliability and validity of EUROQUEST questionnaire in Spain, Marhuenda et al.13 found that the questionnaire had a favorable validity in the Spanish workers’ community, while Cronbach’s alpha was reported to be 0.92. Evaluation of the reliability and validity of the French version of this questionnaire indicates Cronbach’s alpha higher than 0.6 for all sections, except sleep disorders.10 EUROQUEST questionnaire has been also translated into several languages (including Italian, French, Swedish, Norwegian, Finnish, Dutch, Danish, German, Greek, and Spanish). Despite the difficulties in interpreting the self-report data, the questionnaire of neurological symptoms has been successfully applied in epidemiologic studies.12 Carter et al.18 examined the reliability and validity of EUROQUEST questionnaire in the Swedish community and indicated its acceptable validity in this society, while they also reported a high Cronbach’s alpha of 0.7 for this questionnaire.
The results of this study showed that the neurological, psychosomatic, and mood symptoms were the most prevalent in the first quartile, and the symptoms of memory and concentration, tiredness, and sleepiness were the most prevalent in the second quartile. Prevalence of tiredness was higher than other dimensions, so that 28% of participants were in the third and fourth quartiles of this dimension.
Hilt et al.19 examined the prevalence of symptoms in dentists exposed to mercury. Their results showed that the exposed group had worse conditions than the control group for all of the symptoms except for the mood. Chaari et al.11 examined the effects of exposure to mercury in dentists and concluded that neurological and memory symptoms were more prevalent in the study group. Also, the results of the study by Moen et al.20 indicated that there was a prevalence of neurological and psychosomatic symptoms, impairment of memory and concentration, fatigue, and sleepiness in dentists. Thetkathuek et al.21 studied the exposure of workers to organic substances and concluded that the highest prevalence of neurotoxic symptoms was related to neurological and psychosomatic symptoms as well as sleep disorders. Keer et al.14 examined neurotoxic symptoms in mechanics and found that the prevalence of neurological, psychosomatic, mood, memory and concentration symptoms had increased.
Moreover, the results of this study showed that there was no significant relationship between any of the six groups of symptoms and work experience. It may be concluded that exposure to these gases in operating room has its short-term effects, although this conclusion requires further investigation.
Among the many factors that can affect mood, quality of life, quality of sleep, etc., special attention should be paid to exposure to anesthetic gases in operating room personnel, and control methods should be used so that the presence of these gases should not exceed the allowable limit. Also, in people suffering from neurotoxic symptoms, intervention and treatment measures should be taken to prevent the condition from becoming acute.
Some confounding factors such as working hours and shifts were controlled, but there were other confounding factors in this study, such as the quality of sleep, and the amount of perceived job stress, etc., which are among the limitations of this study and should be considered in interpreting the results.
Conclusions
EUROQUEST questionnaire has acceptable validity and reliability and can be used in studies of neurotoxic symptoms. The study of the prevalence of symptoms also indicated that most participants complained about memory and concentration, fatigue, and sleepiness, and these symptoms were observed in all individuals regardless of their work experience.
Acknowledgments
The authors thank all the participants in this study and the Vice President for Research and Technology.
Conflict of Interest
No potential conflict of interest was reported.
Funding
This study was supported by Hamadan University of Medical Sciences [grant number: 9612228372].
References
| 1 |
Handayani R, Abdullah T, Naiem F, et al.
Effects of isoflurane exposure to fertility through estrogen gene expression in operating room nurses.
Am J Public Health Res. 2018;6(1):11-17.
|
| 2 |
Melhado MA, Hensen J, Loomans M, Forejt L.
Review of operating room ventilation standards.
|
| 3 |
Braz LG, Braz JRC, Cavalcante GAS, Souza KM, Lucio LMC, Braz MG.
Comparison of waste anesthetic gases in operating rooms with or without an scavenging system in a Brazilian University Hospital.
|
| 4 |
Casale T, Caciari T, Rosati MV, et al.
Anesthetic gases and occupationally exposed workers.
Environ Toxicol Pharmacol. 2014;37(1):267-274.
|
| 5 |
Yılmaz S, Çalbayram NÇ.
Exposure to anesthetic gases among operating room personnel and risk of genotoxicity: a systematic review of the human biomonitoring studies.
J Clin Anesth. 2016;35:326-331.
|
| 6 |
Neisi A, Albooghobeish M, Geravandi S, Mohammadi MJ, Torabpour M, Hashemzadeh B.
Association of anesthetic toxic isoflurane gases of the indoor air of operating room, Ahvaz, Iran during 2016.
Toxin Reviews. 2017;36(2):141-146.
|
| 7 |
Zare Sakhvidi MJ, Barkhordari A, Salehi M, Behdad S, Fallahzade H.
The assessment of occupational exposure of operation room personnel to isoflurane anesthetic gas.
Occup Med Q J. 2012;4(3):1-9.
|
| 8 |
Scapellato ML, Mastrangelo G, Fedeli U, et al.
A longitudinal study for investigating the exposure level of anesthetics that impairs neurobehavioral performance.
Neurotoxicology. 2008;29(1):116-123.
|
| 9 |
Kaukiainen A, Hyvärinen HK, Akila R, Sainio M.
Symptoms of chronic solvent encephalopathy: Euroquest questionnaire study.
Neurotoxicology. 2009;30(6):1187-1194.
|
| 10 |
Rouch I, Wild P, Fontana JM, Chouaniere D.
Evaluation of the French version of EUROQUEST: a questionnaire for neurotoxic symptoms.
Neurotoxicology. 2003;24(4-5):541-546.
|
| 11 |
Chaari N, Chebel S, Merchaoui I, et al.
Neuropsychological effects of mercury exposure among dentists in Monastir city.
Recent Pat Inflamm Allergy Drug Discov. 2015;9(2):151-158.
|
| 12 |
Chouanière D, Cassitto MG, Spurgeon A, Verdier A, Gilioli R.
An international questionnaire to explore neurotoxic symptoms.
Environ Res. 1997;73(1-2):70-72.
|
| 13 |
Marhuenda D, Prieto M, Cardona A, Roel JM, Oliveras MA.
Transcultural adaptation and validation of the Spanish version of EUROQUEST.
Neurologia. 2015;30(4):201-207.
|
| 14 |
Keer S, Glass B, Prezant B, et al.
Solvent neurotoxicity in vehicle collision repair workers in New Zealand.
Neurotoxicology. 2016;57:223-229.
|
| 15 |
Hyrkäs K, Appelqvist-Schmidlechner K, Oksa L.
Validating an instrument for clinical supervision using an expert panel.
Int J Nurs Stud. 2003;40(6):619-625.
|
| 16 |
Jöreskog KG, Sörbom D.
LISREL 8: User’s Reference Guide.
|
| 17 |
Breckler SJ.
Applications of covariance structure modeling in psychology: cause for concern?
Psychol Bull. 1990;107(2):260-273.
|
| 18 |
Carter N, Iregren A, Söderman E, et al.
EUROQUEST—a questionnaire for solvent related symptoms: factor structure, item analysis and predictive validity.
Neurotoxicology. 2002;23(6):711-717.
|
| 19 |
Hilt B, Svendsen K, Syversen T, et al.
Occurrence of cognitive symptoms in dental assistants with previous occupational exposure to metallic mercury.
Neurotoxicology. 2009;30(6):1202-1206.
|
| 20 |
Moen BE, Hollund BE, Riise T.
Neurological symptoms among dental assistants: a cross-sectional study.
J Occup Med Toxicol. 2008;3:10.
|
| 21 |
Thetkathuek A, Jaidee W, Saowakhontha S, Ekburanawat W.
Neuropsychological symptoms among workers exposed to toluene and xylene in two paint manufacturing factories in eastern Thailand.
Adv Prev Med. 2015;2015:183728.
|