Massive pulmonary hemorrhage can be life threatening. A double-lumen endotracheal tube (DLT) or a bronchial blocker used for lung isolation can preserve ventilation function. However, during a massive pulmonary hemorrhage, identifying an accurate position of endotracheal tube using fiberoptic bronchoscopy is difficult. Here, we present a patient with a massive pulmonary hemorrhage, who successfully underwent mobile digital radiography-guided DLT placement for lung isolation.
The 77-year-old male patient had chronic obstructive pulmonary disease and bronchiectasis and was receiving regular medication. Acute massive pulmonary hemorrhage was noted during his admission to the hospital. There was a persistent decrease in oxygen saturation after endotracheal tube insertion under the impression of right side pulmonary hemorrhage according to previous image studies; hence, we performed DLT placement for lung isolation. Identifying the accurate placement position by fiberoptic bronchoscopy was difficult because blood obstructed the visual field of the bronchoscope, and bilateral diminished breathing sound due to blood occlusion makes DLT adjustment by auscultation difficult. Hence, we performed mobile digital radiography, which immediately provided a chest plain film and identified the bronchial and tracheal cuff positions of DLT and tracheal and bilateral bronchus. The first chest radiography revealed the bronchial tube was remaining in the tracheal, and DLT tip was just above the carina (Fig. 1A ). We adjusted the depth from central incisors of DLT from 27 to 30 cm. The oxygen saturation gradually increased to the normal range, and the patient was sent for angiographic hemostasis where the follow-up plain film showed DLT in the right place (Fig. 1B ). By this method, we could adjust DLT position and shorten the desaturation time. There were no complications such as neurologic defect after angiographic hemostasis.
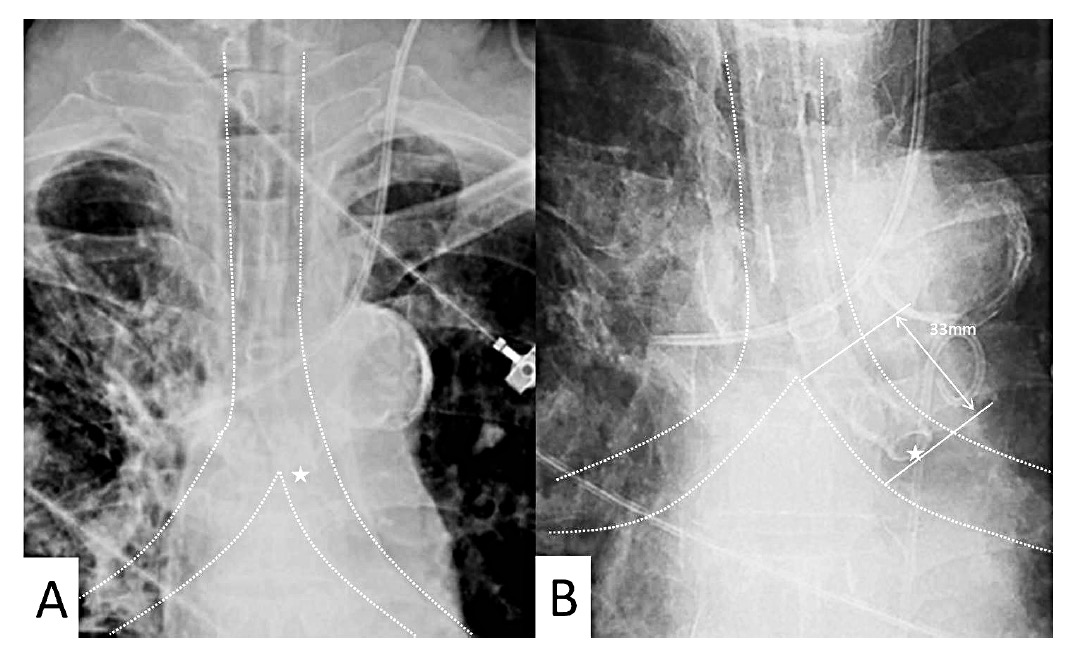
Download full-size image
According to a previous study, most clinicians prefer using a single endotracheal tube over DLT because they lack proficiency in using DLT.1 Currently, several alternatives are available for checking the position of DLT, such as use of video-capable double-lumen tube, sonography, wireless video assistance, and fluoroscopy.2-4 However, most alternative methods, such as fluoroscopy and use of video-capable double- lumen tube, are performed in an operating room and need a unique technique or additional equipment and cannot be immediately performed under general ward settings. Mobile digital radiography, unlike traditional radiography that needs X-ray film processing, can immediately produce the image on its digital display. In this case, based on the images displayed on the mobile digital radiography machine, we adjusted the depth and direction of DLT, despite having blood or secretions accumulated in the airway. This approach could save time and could be performed in a general ward setting. Additionally, this can be a life-saving approach for patients with massive pulmonary hemorrhage requiring lung isolation to preserve ventilation function. Therefore, in such patients, we suggest that early contact with a medical radiation technologist for performing mobile digital radiography is important. This could be an alternative method to assess DLT position as well as to guide DLT placement.
References
| 1 |
Haponik EF, Fein A, Chin R.
Managing life-threatening hemoptysis: has anything really changed?
Chest 2000;118:1431–1435.
|
| 2 |
Heir JS, Purugganan R, Jackson TA, et al.
A retrospective evaluation of the use of video-capable double-lumen endotracheal tubes in thoracic surgery.
J Cardiothorac Vasc Anesth 2014;28:870–872.
|
| 3 |
Ponsonnard S, Karoutsos S, Gardet E, Marsaud JP, Nathan N.
Value of lung sonography to control right-sided double lumen endotracheal tube location.
J Anesth Clin Res 2014;5:453.
|
| 4 |
Calenda E, Baste JM, Hajjej R, et al.
Fluoroscopic guidance for placing a double lumen endotracheal tube in adults.
Acta Anaesthesiol Taiwan 2014;52:107–109.
|